

| Question Everything! |
Covid Is Revealing the Cancerous Underbelly of U.S. Healthcare
By Charles Hugh Smith
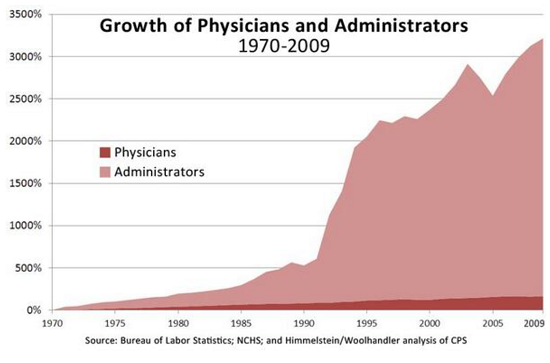
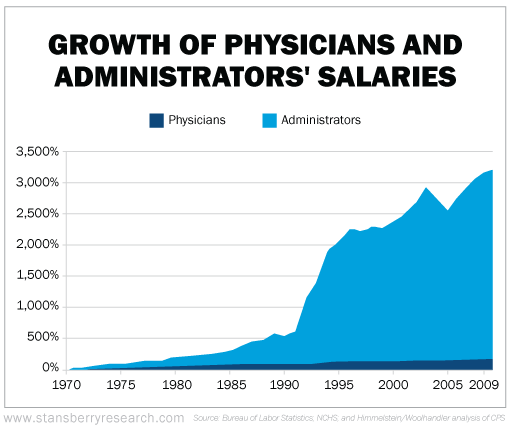
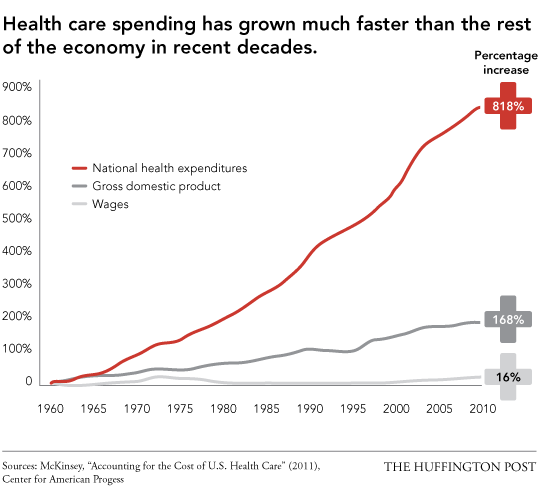
If you still believe that America's Sickcare is "the finest in the world" and is endlessly sustainable, please study these three charts and extend the trendlines.
December 07, 2020 "Information
Clearing House" - I've long
been making the distinction between
healthcare and sickcare:
healthcare is the service provided by
frontline operational caregivers (doctors,
nurses, aides, technicians, etc.) and
sickcare is the financialized system of Big
Hospital Corporations, Big Insurers, Big Pharma,
etc. and their lobbyists that keep the federal
money spigots wide open.
This financialized sickcare system is
being consumed by the cancer of greedy
profiteering pursued by self-serving insiders.
The delivery of healthcare is secondary to
maximizing revenues and profits by any means
available.
To believe such a corrupt system is sustainable
is magical thinking at its most destructive.
Covid-19 is revealing this cancerous underbelly.
Knowledge of the inner workings of corporate
administration is not evenly distributed, so
every participants' experience of the systemic
dysfunction will vary.
Here is one MD's observations of the system's
priorities. Others may have different views but
the maxim follow the money is clearly the
correct place to start any inquiry of how
America's financialized sickcare
functions in the real world.
No Advertising - No Government Grants - No Algorithm - This Is Independent Media
From what I'm hearing from
the front line, a not insignificant number of
admissions are of folks who would not have been
admitted in March when there was fear of both
the unknown and systemic failure and, not
coincidently, when COVID diagnoses didn't pay as
much.
Today, the admission criteria for COVID is so
much more flexible than for standard diagnoses
like CHF, and pays so much better than other
diagnoses that our 'healthcare' system is
rapidly becoming a 'COVID care' system.
The surge in hospitalizations and subsequent
COVID-identified deaths may be driven, in part,
to health systems adapting to new COVID revenue
streams.
This would seemingly be good news, after all if
it's the hospital administrator's desire to fill
empty beds that's driving admissions rather than
infection rates, then systemic failure can be
averted through moderating those admission rates
based on system capacity.
If your hospital fills up, just start sending
the marginal cases home--inpatient/outpatient;
the outcome for the patient will be pretty much
the same and you've made as much money as your
capacity will allow.
Unfortunately, our healthcare 'system' doesn't
work like that.
Health systems are in the business of generating
revenue, not value. Recent COVID-related demand
destruction has crushed that revenue so they're
hungry for more.
Those in health-system operations and those in
leadership live in two different worlds.
Leadership will push COVID admissions far beyond
any operational limits in their quest for short
term performance. One cannot overstate their
mendacity and drive for lucre.
Hospitals are becoming 'COVID factories' with
all other admissions (which pay far less)
relegated to second tier status.
Health systems are evolving into an 'all COVID,
all the time' format with the emphasis on
testing and (soon) vaccination, at the expense
of all else.
Not a few systems of my acquaintance are laying
off outpatient medical staff because their
supporting personnel have quit and are not
replaced--those resources are being re-directed
to COVID testing and in preparation for mass
vaccination.
For the health system in the business of
generating revenue, it's an excellent tactic.
They save themselves significant overhead by not
paying the clinicians and they make up the
revenue through high-margin COVID services and
government bailout payments.
For patients who actually need healthcare,
though, this tactic is deadly.
The perversion is end-stage, the health systems
pretend to deliver healthcare and the government
pays them to continue the pretense.
There is no long term thinking here, no empathy
for the workforce, no thought to the mission
beyond window-dressing--just a relentless,
risk-adverse financialization machine.
Think of COVID as a new widget for which the
customer will pay 2.5 times the going price with
no quality control, but only for a limited
amount of time. Add in talentless, rent-seeking
leadership and all becomes clear.
Of course the real risk is that maxed out
hospitals could find themselves in a situation
where admissions suddenly become driven by
demand rather than the business model, with a
true non-linear path to failure laying beyond.
The longer daily national hospital occupancy
stays above the approximate pre-COVID capacity
of 100k, the more likely you'll see systemic
breakdowns--local at first, then regional.
You won't see it in the press, the healthcare
cartels have a pretty good lock on the local
media. Once news starts getting censored on
social media, though, then you know it's
happening.
Hold me to that, And call me out in three months
if I'm not right.
If you still believe that America's
sickcare is "the finest in the world" and is
endlessly sustainable, please study these three
charts and extend the trendlines.
Charles Hugh Smith is the
proprietor of the popular blog
OfTwoMinds.com.
His new book is
A Hacker's Teleology: Sharing the Wealth of Our
Shrinking Planet 20% and 15% discounts
(Kindle $7, print $17) -
Read excerpts of the book for free (PDF).
-
The Story Behind the Book and the Introduction.